 |
Clinical evaluation of the orbit involves three critical steps: (1) taking a detailed history; (2) conducting a clinical exam of the extraocular muscles (EOMs), assessing resistance to retropulsion and performing exophthalmometry; and (3) performing imaging of the orbit and brain with computed tomography (CT) or magnetic resonance imaging (MRI). Acute symptoms of diplopia, vision loss, proptosis and hyperemia are often associated with inflammation, infection, vascular anomalies and, occasionally, tumors. Each of these conditions will be presented in a stepwise fashion based on presenting factors.
 |
| This is a subconjunctival heme from a gunshot injury. |
Scenario 1: Acute painful proptosis and hemorrhage. A patient with severe subconjunctival hemorrhage and chemosis can be a diagnostic challenge. Although most cases present in the setting of trauma, post-op status and prolonged anticoagulation therapy are risk factors.
The most important condition to consider in this setting is retrobulbar hemorrhage. If a history of trauma exists, the patient should be evaluated for an open-globe injury. Evidence of rupture warrants application of a plastic shield to the affected eye and immediate transport to the closest emergency department (ED) for surgical repair. In the setting of a closed-globe injury, measure intraocular pressure and evaluate EOMs and posterior segment to determine the extent of retro-orbital involvement and risk of optic nerve compression or avulsion. Following the clinical examination, urgent emergent non-contrast orbital CT is the most appropriate modality to assess for structural damage.
Scenario 2: Acute or subacute painful proptosis, chemosis and diplopia. The three most common conditions that present similarly include orbital inflammatory syndrome (OIS), orbital cellulitis and arteriovenous malformation (AVM). Infectious causes of unilateral painful proptosis are uncommon and include cellulitis and mucormycosis.
• OIS. This is a disorder of the orbit characterized by a polymorphous lymphoid infiltrate with varying degrees of fibrosis.1 In a review, the most common orbital component affected was intraconal fat, followed by lacrimal gland enlargement and EOM restriction. To determine the level of soft tissue involvement, it’s best to evaluate OIS with contrast-enhanced orbital MRI.2
OIS is associated with autoimmune diseases such as Crohn’s disease, systemic lupus erythematosus, rheumatoid arthritis, granulomatosis with polyangiitis and sarcoidosis. The first-line therapy for OIS is systemic corticosteroids; 75% of cases show improvement within 24 to 48 hours. An initial dose of 60mg to 80mg of oral prednisone should be started after MRI is used to discount alternative etiologies such as orbital cellulitis and lymphoma.3
• Orbital cellulitis. The clinical characteristics of this condition include fever and antecedent sinusitis, periorbital swelling with proptosis, conjunctival hyperemia with chemosis and EOM restriction. Management involves emergent referral to the ED for immediate intravenous broad-spectrum antibiotics including a third-generation cephalosporin and the narrow-spectrum penicillin class antibiotic flucloxacillin, which are effective against Staphylococcus aureus, Staphylococcus epidermidis, Streptococci and Haemophilus species.
Next, order non-contrast CT of the brain and orbits to demonstrate an infective source in order to obtain cultures, evaluate for intracranial extension and assess the need for surgical drainage. Surgery is indicated for significant sinus disease, including orbital or subperiosteal abscess.4
• Mucormycosis. This is an aggressive opportunistic fungal infection that enters through the paranasal sinus mucosa and travels to the orbital apex, where it can breach the intracranial space. A patient with acute symptoms should undergo emergent referral to the ED for non-contrast CT of the head, orbit and sinuses to assess the extent of the disease process followed by biopsies of involved tissues and sinus mucosal secretions. Those with less aggressive signs can be managed on an outpatient basis with contrast-enhanced MRI of the sinuses, orbit and brain. Early MRI findings include lack of enhancement within the sinus mucosa and cavernous sinus, a finding consistent with devitalized tissue. First-line medical therapy includes amphotericin B and counteracting the potential sequelae of acidemia and hyperglycemia with IV insulin and fluids.5
• Arteriovenous malformations. These are high-flow or low-flow communications between arteries and veins with no interposed capillary bed; the most common are carotid-cavernous fistulas (CCF).6 AVM can be classified as traumatic vs. spontaneous, high-flow vs. low-flow, and direct vs. dural.
The clinical scenario of acute unilateral proptosis with severe chemosis, pain, orbital bruit, restricted ocular motilities, elevated IOP and dilated episcleral veins suggests a high-flow fistula from trauma or an aneurysmal rupture of the internal carotid artery within the cavernous sinus, necessitating emergent imaging of the brain and orbits.7 Contrast-enhanced magnetic resonance angiography (MRA) and CT angiography are superior for evaluating venous distention, the lumen of aneurysms and increased flow to the cavernous sinus. Surgical treatment with embolization is warranted when optic nerve compression exists or when congestion from the superior ophthalmic vein and cavernous sinus places the cerebral venous circulation at risk for thrombosis.
The other CCF form is classified as low-flow. Astute clinical evaluation is essential because the signs and symptoms are relatively mild and often overlooked in favor of more benign entities such as ocular surface disease, conjunctivitis or episcleritis. Contrast-enhanced MRI or MRA of the head and orbit is the preferred imaging modality. Most lesions undergo spontaneous occlusion without visual sequelae.8
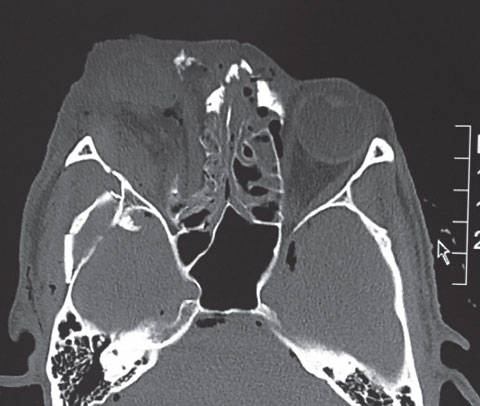 |
| Here is a CT image of the gunshot injury. |
Scenario 3: Intermittent Pain and Proptosis. The clinical presentation of a young adult with complaints of intermittent positional pain and proptosis exaggerated during valsalva-type maneuvers should be initially evaluated with non-contrast CT, for an enlarged superior ophthalmic vein consistent with orbital varices.9
Varices are venous malformations that consist of low-pressure and low-flow plexi that intermingle within the orbital circulation. If the clinical history is suspicious for varices and CT imaging is normal, magnetic resonance venography (MRV) should be performed to evaluate the orbital and intracranial venule system. While surgery is reserved for varices that cause significant pain, proptosis and optic nerve compression, small lesions with minimal signs and symptoms can be observed.10
Scenario 4: Painless Progressive Proptosis. Suspect cavernous hemangioma in these circumstances. This is the most common orbital tumor in adults and typically presents in middle age with painless, progressive proptosis that causes hyperopia and choroidal folds. The differential diagnosis includes orbital metastasis, orbital lymphoma and hemangiopericytoma. While most orbital processes are best evaluated with MRI, progressive signs of proptosis, optic neuropathy and choroidal folds often signal a retro-orbital mass, easily identifiable with non-contrast orbital CT.11 Lesions causing significant proptosis, optic neuropathy or visually significant choroidal folds should be surgically removed.
Unilateral proptosis often presents a diagnostic dilemma. However, taking a detailed history, performing a comprehensive clinical exam and using appropriate neuroimaging techniques will help rule out emergent causes and increase the chance of early diagnosis for the patient.
| 1. Orbits, Eyelids, and Lacrimal System. Basic Clinical Science Course, Section 7. San Francisco: American Academy of Ophthalmology; 2011-2012:59. 2. Swamy BN, McCluskey P, Nemet A, et al. Idiopathic orbital inflammatory syndrome: Clinical features and treatment outcomes. Br J Ophthalmol. 2007;91:1667-70. 3. Mombaerts I, Goldschmeding R, Schlingemann RO, Koornneef L. What is orbital pseudotumor? Surv Ophthalmol. 1996;41:66-78. 4. Chaudhry IA, Shamsi FA, Elzaridi E, et al. Outcome of treated orbital cellulitis in a tertiary eye care center in the Middle East. Ophthalmology. 2007;114:345-54. 5. Kauh CY, Nelson CC. Diagnosis and management of orbital mucormycosis. EyeNet Magazine. June 2014. 6. Levy JV, Zemek L. Ophthalmic arteriovenous malformations. Am J Ophthalmol. 1966;62:971-4. 7. Gean AD. Imaging of Head Trauma. New York, NY: Raven Press;1994:349-54,474. 8. Flanagan JC. Vascular problems of the orbit. Ophthalmology. 1979;86:896-913. 9. Shields JA, Dolinskas C, Augsburger JJ, et al. Demonstration of orbital varix with computed tomography and valsalva maneuver. Am J Ophthalmol. 1984;97:108-10. 10. Islam N, Mireskandari K, Rose GE. Orbital varices and orbital wall defects. Br J Ophthalmol. 2004;88:1092-1093. 11. Thorn-Kany M, Arrue P, Delisle MB, et al. Cavernous hemangiomas of the orbit: MR imaging. J Neuroradiol. 1999;26(2):79-86. |
