 |
DED Treatment: A Combined Effort
In response to the rising prevalence of DED, manufacturers have brought a variety of new pharmacological treatment options to market, including tear substitutes, eyelid therapeutics, dietary supplements and anti-inflammatory agents.1 But successful treatment of DED typically requires multiple treatment platforms targeting each patient’s particular combination of symptoms, signs and severity. For instance, tear replacement—although highly effective—is rarely successful when used as the sole treatment.2 However, when combined with other therapies, such as changes to the patient’s environment, the use of anti-inflammatory medications, treatment of the obstructed glands and biofilm control, patients are more likely to achieve improvement.
With so much to choose from, we tend to overlook the tried-and-true lacrimal occlusion for the treatment of DED and contact lens intolerance secondary to dry eye. It can increase the efficacy of ocular co-treatment medications and lubricants by allowing medications to stay on the eye longer or increasing contact time.
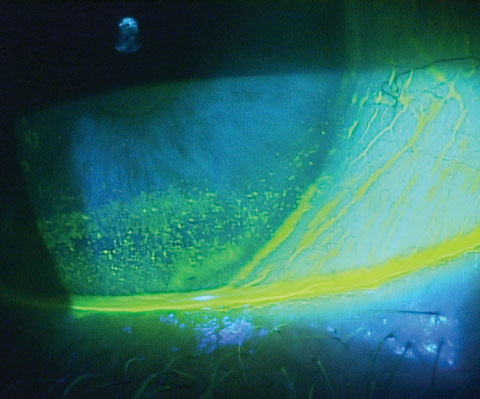 |
| Patients with inferior corneal staining secondary to lagophthalmos, as seen here, are good candidates for punctal occlusion. |
Plugging it Up
For some patients, punctal plugs should be the first line of treatment. Patients with neurotrophic dry eye are ideal candidates for punctal occlusion, as are patients with contact lens intolerance due to early DED. Neurotrophic dry eye, often caused by conditions such as herpes zoster ophthalmicus or diabetes, often affects patient’s nerves, resulting in poor communication between the lacrimal functional unit and the brain. Patients typically do not have an inflammatory, or any, response, which is why the eye continues to remain desiccated or have a persistent epithelial defect.3,4 Therefore, it’s likely punctal plugs would simply elevate the tear volume, which is critical to improving this form of DED.5Punctal plugs can be a particularly well-suited option for those with lagophthalmos with inferior corneal staining, as the elevation of the tear lake after punctal occlusion is often enough to clear the lower area of ocular irritation.
Finally, punctal plugs provide a means by which ODs can address drop noncompliance. Research shows punctal occlusion can increase the efficacy of drops and increase therapeutic effect by allowing a greater contact time of the medications.6 In one study, patients were randomized to cyclosporine alone, punctal plugs alone and punctal plugs with cyclosporine. Although all three groups improved, the group that had both therapeutics and punctal plugs had the longest period of ocular surface health and improved symptoms, suggesting treatment may be additive.6
No Plug, Please
As with all treatment modalities, there are contraindications to punctal occlusion. Patients with an active infection, abnormal drainage of the lacrimal system or sensitivity to the material are not candidates. Clinicians should also avoid punctal plug use in cases of allergic conjunctivitis, where occluding the punctae could result in the allergens remaining on the ocular surface and possibly increasing the allergic response. Punctal plugs are not optimal for patients with significant blepharitis who need the biofilm removed with mechanical treatments such as Blephex (RySurg) and lid scrubs.Finally, clinicians should first treat advanced levels of inflammation on the ocular surface with topical therapies, omega fatty acids or oral doxycycline before considering punctal occlusion. Once inflammation is controlled or the biofilm is treated, punctal plugs are once again a possible treatment option.
New Technologies
New innovations have made punctal occlusion a therapeutic option for any number of indications. Absorbable plugs that dissolve over an approximately 90- or 180-day period—e.g., Comfortear Lacrisolve 180 absorbable punctum plugs (Paragon BioTeck), Extend absorbable synthetic implants (Beaver-Visitec), Quintess six-month dissolvable lacrimal plug (OcuSoft)—can provide a huge benefit to patients in need of DED relief.The plugs are easy to insert in office and sit completely under the surface, posing little risk to the patient. While an excellent treatment tool for DED, they can also serve as a diagnostic tool to help clinicians determine the patient’s response to occlusion therapy. Patients who respond well to the 180-day plug are often good candidates for long-term silicone punctal plugs.
However, I have found that many patients notice continued relief even after the 90- or 180-day plugs absorb, and I simply replace them with another extended duration plug months later if symptoms return.
 |
| Bruder punctal plug forceps have a grove for easily grasping the plugs and are particularly useful for collagen and extended duration plugs. |
Safety and Efficacy
Multiple studies confirm the efficacy of punctal plugs compared with topical treatment alone. A prospective double-masked study demonstrated a 94.2% reduction in dry eye symptoms and 93% reduction in conjunctival symptoms eight weeks after lacrimal occlusion.7 The control group remained unchanged. Additionally, nearly 77% of the occlusion therapy subjects were virtually symptom free, and 100% of the participants no longer required moisturizing drops.7A 2016 study evaluating 29 patients with moderate dry eye also showed significant symptomatic relief and reduced fluorescein staining in all except the inferior corneal zone three weeks following punctal occlusion.8 Although patients had significant symptomatic improvement and improved staining, tear analysis showed minimal effect on tear cytokines and MMP-9 levels. This suggests a need for dual treatment (plugs and anti-inflammatory medications) earlier in dry eye management.8
Research is underway on drug-eluting punctal plugs that contain either corticosteroids or cyclosporine. We may in the future have an option that provides punctal occlusion with slow-release therapeutic medications.
An observational study of silicone plugs indicated a satisfactory retention rate of 84.2% after three months, 69.5% after one year and 55.8% after a median of two years (17 to 93 months) with few complications.9
Further, with a mean retention period of 85 weeks, patients opting for punctal plugs can look forward to living an extended period relatively free of dry eye symptoms.10
With a plethora of new options to address dry eye symptoms, we should not overlook the benefits of occlusion therapy. Patients suffering from chronic DED will embrace the opportunity for a long-term treatment option and, quite likely, rejoice at the prospect of eliminating or reducing the frequency of instilling lubricating agents.
Dr. Karpecki is a consultant to Beaver-Visitec, Blephex, Ocular Therapeutix, OcuSoft, Bruder and Paragon BioTeck.
| 1. Paulsen AJ, Cruickshanks KJ, Fischer ME. Dry eye in the beaver dam offspring study: prevalence, risk factors, and health-related quality of life. Am J Ophthalmol. 2014 Apr;157(4):799-806. 2. Stern ME, Beuerman RW, Fox RI, et al. The pathology of dry eye: the interaction between the ocular surface and lacrimal glands. Cornea. 1998 Nov;17(6):584-9. 3. Schulte-Herbrüggen O, Braun A, Rochlitzer S, et al. Neurotrophic factors––a tool for therapeutic strategies in neurological, neuropsychiatric and neuroimmunological diseases? Curr Med Chem. 2007;14(22):2318-29. 4. Chen HJ, Pires RT, Tseng SC. Amniotic membrane transplantation for severe neurotrophic corneal ulcers. Br J Ophthalmol. 2000 Aug;84(8):826-33. 5. Tai MC, Cosar CB, Cohen EJ, et al. The clinical efficacy of silicone punctal plug therapy. Cornea. 2002 Mar;21(2):135-9. 6. Roberts CW, Carniglia PE, Brazzo BG. Comparison of topical cyclosporine, punctal occlusion, and a combination for the treatment of dry eye. Cornea. 2007 Aug;26(7):805-9. 7. Nava-Castaneda A, Tovilla-Canales J, Rodriquez L, et al. Effects of lacrimal occlusion with collagen and silicone plugs on patients with conjunctivitis associated with dry eye. Cornea. 2003;22(1):10-4. 8. Tong L, Beuerman R, Simonyi S, et al. Effects of punctal occlusion on clinical signs and symptoms and on tear cytokine levels in patients with dry eye. The Ocular Surface. 2016 Apr;14(2):233-41. 9. Horwath-Winter J, Thaci A, Gruber A, et al. Long-term retention rates and complications of silicone punctal plugs in dry eye. Am J Ophthalmol. 2007;144(3):441-4. 10. Tai M, Cosar C, Cohen E, et al. The clinical efficacy of silicone punctal plug therapy. Cornea. 2002;21(2):135-9. |
